In this episode I’ll:
1. Review the FDA briefing documents for sugammadex
2. Answer a drug information question about dabigatran
3. Share a great resource I use for evaluating drug interactions
Subscribe on iTunes, Android, or Stitcher
Before we get to the topic for today’s show I want to invite you to join the Pharmacy Nation Slack group. This is a free group with other pharmacists from around the world collaborating with each other using real-time messaging to help better care for patients. I hope you join me and the over 85 other Pharmacy Nation members there! You can sign up at pharmacynation.org.
Article
Even though they are not published in a peer-reviewed journal, FDA briefing documents are a treasure trove of information. In these documents you can read FDA expert opinions as they analyze published and unpublished data about new medications seeking FDA approval. Reviewing these briefing materials can give you an in-depth understanding of the risks and benefits of new medications that you won’t be able to find in the prescribing information or even published articles in medical journals.
I know I’m dating myself here, but do you remember when rofecoxib was recalled in 2004? The events surrounding the recall of rofecoxib involved the purposeful non-reporting by the manufacturer of adverse cardiac events with the medication. The medication was on the market for 5 years before the “discovery” of the cardiac risk led to its withdrawal. But the concern for cardiac adverse events was well documented in the 2001 FDA briefing materials for rofecoxib. Anyone who read these documents would have been able to see it, but these documents are seldom reviewed by prescribers or other health care practitioners.
Also made routinely available on the FDA website are transcripts of the FDA advisory committee meetings – these can also provide fascinating insights into new medications by the questions & answers experts provide at the advisory committee meetings.
The documents are sometimes hundreds of pages long, so don’t go to the FDA website if you are looking for leisure reading material!
So when I heard that the 2015 Anesthesia FDA advisory committee recommended the approval of sugammadex, one of the first things I checked out was the FDA briefing material. Here is what I learned:
Sugammadex is in the γ-cyclodextrin class of medications. It was designed to bind rocuronium and vecuronium for the purpose of reversing paralysis from these neuromuscular blocking medications.
Unlike neostigmine (which also reverses neuromuscular blockers), sugammadex does not inhibit acetylcholinesterase. This means cholinergic effects are not produced and glycopyrrolate or atropine does not need to be co-administered.
In 2008, the FDA rejected a New Drug Application for sugammadex due to concerns over hypersensitivity. It was approved for use in the European Union on July 29, 2008.
The 2015 FDA advisory committee documents detail concern about hypersensitivity to sugammadex, as it has been detected in several pre-approval studies of the drug. The concern was significant enough that the anesthesia advisory committee asked for the FDA’s allergy advisory committee to provide their opinion of the allergy risks for sugammadex.
The review provided in advisory committee documents concludes that sugammadex does cause hypersensitivity reactions and anaphyalxis. The reviewers go on to say that IgE antibodies are not produced, and repeat exposure does not seem to increase the risk of hypersensitivity. Ultimately, the risk-benefit assessment for sugammadex depends on the efficacy and safety data specific to sugammadex and its expected use in a real-world setting.
There is much more to learn about this soon-to-be-new-to-the-US medication, and I’ve linked some articles on the dosing & efficacy of sugammadex as well as a case report describing sugammadex reversing anaphylaxis to rocuronium that was not responding to traditional treatment.
Drug information question:
Q: Do I need to reduce the dose of dabigatran for a patient with a creatinine clearance of 40 mL/min?
A: It depends.
Thank goodness for Praxbind (covered in episode 31)! Dabigatran has got to have the most confusing renal adjustment parameters of any medication I’ve encountered. Renal dose adjustment for dabigatran depends not only on the kidney function but also on the indication for its use! For patients on dabigatran for DVT or PE and a creatinine clearance of 40 mL/min, no dose adjustment is necessary unless the patient is also receiving a PGP inhibitor. For patients on dabigatran for nonvalvular atrial fibrillation (afib) and a creatinine clearance of 40 mL/min, no dose adjustment is necessary unless the patient is on dronaderone or ketoconazole. No adjustment is recommended even though the area under the curve for dabigatran may be increased three-fold for a patient with this level of kidney function!
The patient in this question was a 72 y/o male taking dabigatran for nonvalvular afib. Even though he wasn’t on dronaderone or ketoconazole (and therefore no dose adjustment was indicated) I still wanted to review his concomitant medications to determine whether he was also on a PGP inhibitor. His other meds were:
albuterol/iptratropium via nebulizer
atenolol
budesonide via nebulizer
celecoxib
furosemide
levofloxacin
methylprednisolone
pantoprazole
risperidone
rosuvastatin
sitagliptin
I wanted to quickly find out whether this medication list included a PGP inhibitor…
Resource
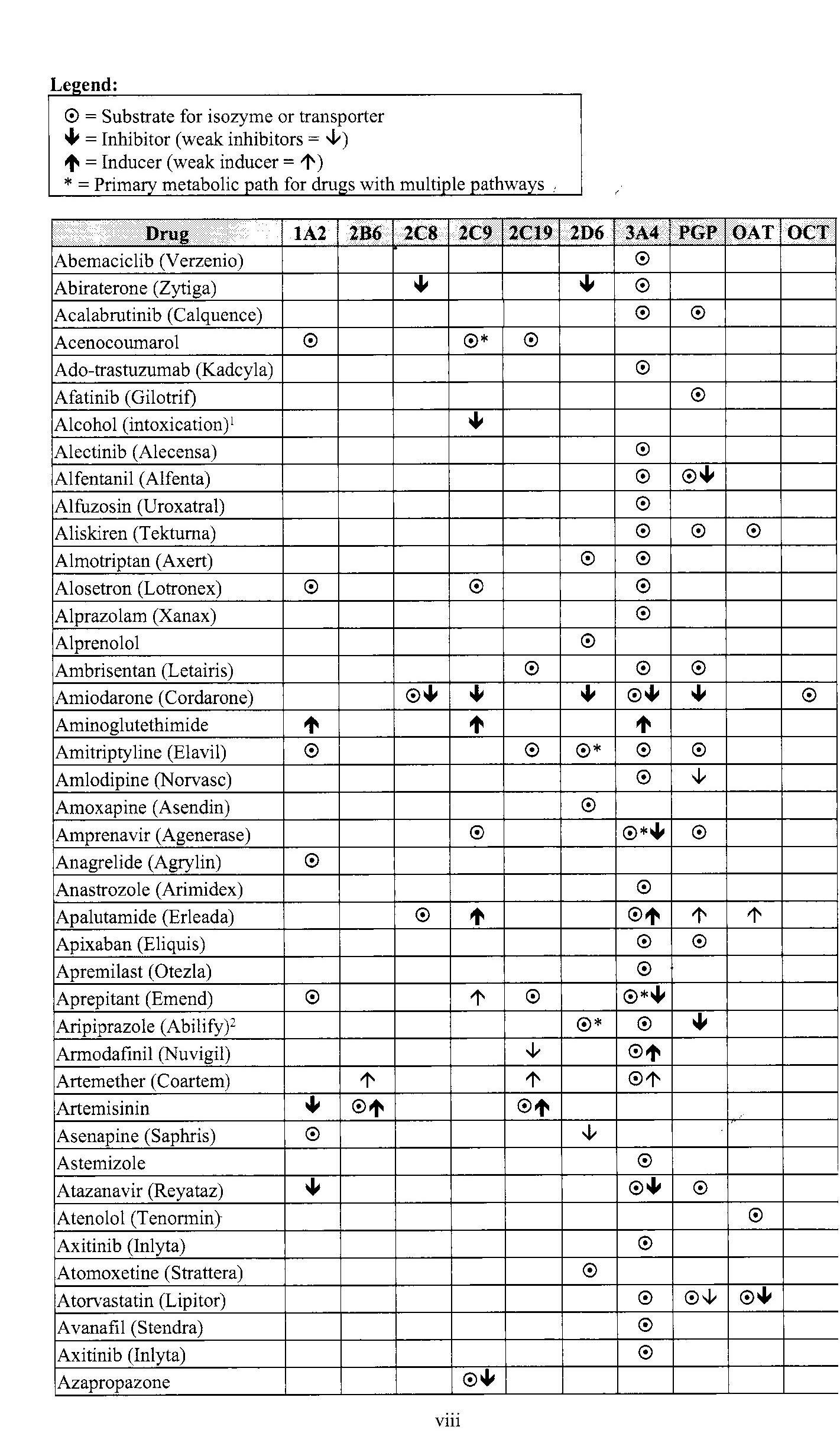
In my labcoat pocket I keep a copy of Hansten & Horn’s Top 100 Drug Interaction Handbook. I’ve praised this book before in episode 12 for its no-nonsense approach to evaluating QTc interactions. This book also happens to include a fantastic chart that lists all of the known CYP450 and PGP inhibitors, inducers, and substrates. In about a minute, I was able to scan the chart to confirm that the patient was not receiving any PGP inhibitors. This book is well worth the $20, as well as the space it takes up in my labcoat every day.
{kind=link}
Since I’ve started this podcast, I’ve noticed there are a lot of pharmacists and other medical professionals sharing their expertise with the world using blogs, Facebook pages, and Twitter accounts. But there are only a handful of high quality medical podcasts that are being published regularly. I’m hoping to change that. That’s why I’m putting together a step-by-step course on how to start a medical podcast – so that other medical professionals can bring their knowledge, expertise, and voice to the world of podcasting. To learn more about the course, and to sign up to be notified when it is available, head over to howtostartamedicalpodcast.com.
If you like this post, check out my book – A Pharmacist’s Guide to Inpatient Medical Emergencies: How to respond to code blue, rapid response calls, and other medical emergencies.
Leave a Reply